



Effective Management of Diabetic Foot Complications

Aug 16, 2023

Dr Tan Yih Kai
The Growing Diabetes Epidemic in Singapore: The Challenges
Diabetes is a growing epidemic in our nation and globally. The prevalence of diabetes among Singapore residents (Singapore citizens and permanent residents) has increased over the past decade. In Singapore, it is estimated that 1 in 9 adults has diabetes. Today, there are over 450,000 Singaporeans living with diabetes. This number is projected to go up to 1 million by 2050 if nothing is done. The Ministry of Health (MOH) launched the War on Diabetes in 2016 in response to the significant health and societal burden posed by diabetes. The cost burden of diabetes, including loss of productivity, is anticipated to double from S$940 million in 2014 to S$1.8 billion in 2050.
People with diabetes are at high risk of developing a range of serious complications, including heart disease, kidney failure, blindness, and lower-extremity complications. The most disabling of these is the lower limb complications. It is the leading cause of diabetes-related hospitalisations and lower limb amputations. In addition to high healthcare costs, it is also associated with a significant reduction in quality of life.

Diabetes Complications
Diabetic Foot Complications
Approximately 25% of diabetics will develop a foot wound or ulcer in their lifetime. Amputation in people with diabetes is 10 to 20 times more common than in people without diabetes. Every year, more than one million leg amputations are performed globally because of diabetes, which is equivalent to one leg amputation every 30 seconds.
In a person with diabetes, higher than normal sugar levels in the body will, over time, damage nerves (neuropathy) and cause blood vessels of the leg and foot to narrow and harden (atherosclerosis), leading to reduced blood flow down to the feet (Peripheral Arterial Disease (PAD)).
a) Diabetic neuropathy:
Diabetic neuropathy can lead to
i) Poor sensation in the feet: Minor injuries to the foot can be left undetected because of poor sensation and may consequently lead to foot ulceration and infection.
ii) Foot deformities: Structural changes in the foot, such as hammertoes, claw toes, the collapse of the midfoot (Charcot’s foot), and limited joint mobility, can result in focal areas of high pressure on the sole. Skin can break down over pressure points, leading to ulceration.
iii) Decreased sweating: Nerves supplying the sweat glands stop functioning, leading to dry, flaky, and cracked skin. Cracked skin in the foot may allow bacteria to enter and cause infection.
b) Peripheral Arterial Disease (PAD):
People with diabetes are at increased risk of atherosclerosis, which narrows and hardens the blood vessels of the leg and within the foot. Poor blood supply to the foot will lead to poor healing and gangrene, as well as a reduced ability to fight infection.

Atherosclerosis with narrowing of an artery
Here are some statistics on diabetic peripheral arterial disease:
- 70% of diabetic wounds have associated PAD
- An ulceration precedes nearly 85% of diabetes-related amputations. This implies that the majority of the amputations can be prevented.
- Two-thirds of elderly patients undergoing amputation do not return to independent life
- About 70% of amputees will die within 5 years
c) Immunocompromised: A poor immune system reduces the ability to combat infection. Small injuries to the foot, such as cuts, blisters, and ingrown toenails, can become infected easily if left untreated. The combination of neuropathy, PAD and poor immunity is responsible for the increased risk of developing foot complications such as ulcers, gangrene, and infection, which may eventually lead to leg amputation if treatment is not sought early.

Skin cracks

Callus
Diabetic foot deformity Photos


Hammer toes


Claw toes

Flat foot

Amputation

Diabetic Foot Wounds and Ulcers

Gangrene

Infected Wounds

Neuropathic (Pressure) Ulcers
Management of Diabetic Foot Complications
It is important to recognize that most diabetic foot complications are manageable, and amputation can be prevented if treatment is sought early. Delayed treatment of diabetic foot complications is common. The main reasons are an underestimation of the severity of foot problems and a lack of recognition of poor circulation. Management of diabetic foot problems is often complex, and experts from other specialities, including vascular/ endovascular surgery, diabetology, and podiatry, may need to be involved.
Successful management of diabetic foot ulcers/wounds hinges on addressing the following treatment modalities:
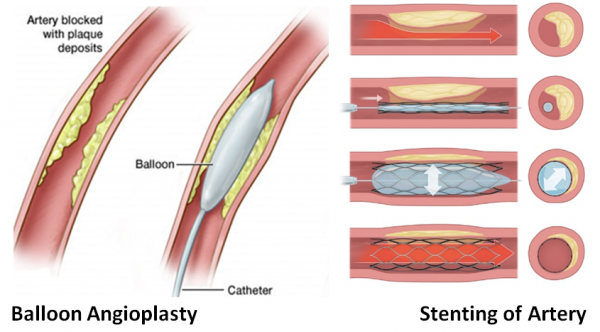
- Ensure adequate blood supply to the foot. Every foot ulcer/wound should be examined for the presence of ischaemia. If poor circulation of the foot is suspected, investigations such as an ultrasound scan or CT angiogram are required to assess the nature of the blockage in the leg arteries. Procedures to improve blood supply to the leg include surgical bypass or endovascular techniques (balloon angioplasty with or without a stent). The treatment of choice depends on the specific type of blockage, which artery is involved, and the general health condition of each patient.
- Control of infection: Signs of wound infection may include:
- Peri-wound redness or swelling
- A foul-smelling wound
- Pus
- Pain
Systemic signs of infection may include fatigue, fever, tachycardia (an increased heart rate), and general malaise. When infection is clinically present, cultures should be obtained. Depending on the infection’s severity, antibiotics shown to be effective against the offending bacteria through sensitivity testing should be given either orally or intravenously.
For a severe wound infection with significant tissue destruction involving muscle, tendon, and bone; urgent surgical intervention will be needed to control the spread of the infection.
- Wound care
- Debride all non-viable tissue (e.g. callus, foreign bodies and necrotic tissue) that may impede wound healing
- Appropriate dressing choice to ensure a moist wound environment for healing.
- Antimicrobial dressings need to be considered to treat and prevent wound infection
- Offloading: redirecting weight (or pressure) off and away from the wound with proper footwear. Some patients may require wheelchairs or crutches to achieve effective offloading.
Prevention
Management of risk factors
- Blood sugar level: High blood sugar, the hallmark of diabetes, injures nerves and blood vessels throughout the body.
- High blood pressure: high blood pressure damages blood vessels, leading to atherosclerosis
- High cholesterol levels and the accumulation of cholesterol-rich fatty deposits in arteries can result in atherosclerosis.
Lifestyle modification
- Smoking cessation: Smoking interferes with blood circulation, and so compounds the effects of nerve and blood vessel damage.
- Exercise naturally improves circulation while working to lower cholesterol and improve heart function.
- Healthy diet: Avoiding excessive salt and saturated fats can help you manage your body weight, blood pressure, and cholesterol.
- Weight loss improves the body’s ability to control blood sugar and takes some pressure off the feet.
Foot Care
- Check your feet and toes every day for cuts, sores, corns or blisters
- Never go barefoot. Choose shoes that are comfortable and fit well. Ill-fitting shoes can cause corns and calluses, ulcers, and nail problems.
- Wash your feet daily. Apply moisturising skin lotion to feet to prevent dryness and cracks.
- Cut or file your toenails regularly.
- Yearly foot screening by a podiatrist, doctor, or trained nurse: Early identification of those at risk of diabetic foot ulcers will prevent the development of foot complications and thus reduce the number of amputations.Education on proper foot care and good glycaemic (blood sugar level) control

Finally, if there are symptoms of unusual pain, redness in the foot, swelling, injury to the foot, infection, or ulcer; make sure this is checked by your doctor or diabetic nurse as soon as possible. There is a clear need to recognise decreased perfusion or vascular impairment as an indicator of the need for revascularization in the diabetic foot in order to achieve and maintain healing and to avoid or delay a future amputation. Early identification of the problem and treatment before it becomes severe is CRITICAL to preventing limb loss.


