




Dive into our comprehensive guide on compression stockings: their role, benefits, and best practices for managing venous diseases effectively and comfortably
How do Compression Stockings Work?
Compression stockings are designed to provide external, consistent, and graduated pressure in the legs, helping blood to flow back to the heart. They are able to improve varicose vein-related symptoms such as pain, the sensation of heaviness, swelling, and night cramps. Compression stockings exert higher pressure at the ankle and lower pressure gradually towards the knee and thigh to ensure blood in the veins is pushed upwards towards the heart.
Compression Stocking Classes, Types, and Sizing Guide
Classes of Compression Stockings
The compression pressure that the garment applies at the ankle level determines the classification of compression stockings. There are four compression classes. The higher the class, the stronger the compression.
| Compression Class | Pressure in mmHg | Indications |
| I | 18–21 | Prevention of DVT Mild varicosities, eg spider veins |
| II | 23–32 | Varicose veins Mild oedema |
| III | 34–46 | Ulcer treatment Post-thrombotic syndrome |
| IV | > 49 | Severe lymphedema |
Types of Compression Stockings
- Knee length
- Thigh length
- Pantyhose
Measurement for Compression Stockings
The sizes of compression stockings will be determined based on measurements of the ankle, calf, and thigh circumferences. A good fit is necessary to ensure that the stockings exert an even pressure. There is no universally accepted sizing method for compression stockings. Measurements need to be taken according to the sizing system of the respective brand of stockings.
Why do Compression Stockings Need to be Prescribed by a Doctor?
Compression stockings are generally safe to wear. However, doctors must prescribe all compression stockings with a compression pressure greater than 20 mmHg. If compression stockings are applied to legs with impaired arterial circulation, they will worsen the ischaemia, which may lead to tissue necrosis or gangrene.
Furthermore, poorly fitted compression stockings can cause more discomfort and pain. Undersized stockings will leave marks on the skin and, at worst, cause skin necrosis. Oversized stockings will cause the stockings to continue sliding down from the top, resulting in ineffective compression.
When and How Long Should I Wear Compression Stockings?
Compression stockings should be worn during the day and removed before going to bed. They should be put back on again first thing in the morning. This is when the leg swelling is minimal, allowing stockings to go up the legs more easily. It is advisable to wear stockings for 4-6 weeks after varicose vein surgery.
How Long Would a Pair of Compression Stockings Last?
Medical-grade compression stockings that are worn and washed daily should maintain their compression effect for about six months. It is advisable to change the stockings every six months. Remember that a pair of worn-out and non-stretchy socks will lose their medical benefits in preventing deep vein thrombosis (DVT), leg swelling, leg ulcers, or venous insufficiency.
Should I also Wear my Medical Compression Stockings Overnight in Bed?
It is ok to wear compression stockings overnight, but it is generally not necessary. Please discuss this with your doctor before doing so. In an upright position, compression stockings provide a constant amount of pressure to the venous circulation system to fight gravity and pump the blood back to the heart. However, when lying down flat in a horizontal position, veins are not subject to gravity pull, and the blood will flow naturally back to the heart. Therefore, the benefit from the compression stockings is minimal. Furthermore, wearing compression stockings at night may apply unnecessary pressure to the ankle, reducing blood supply to the leg, especially in those who already have poor arterial circulation.
What Are Some Tips to Help When Putting Compression Stockings On?
Putting compression stockings on and taking them off can be challenging, especially for the elderly and those with arthritis. There are a variety of tools available on the market to help with putting on and taking off compression stockings. These include:
FAQs
Do compression stockings contain latex?
Most brands of compression stockings are latex-free. Please ask your doctor to ensure that the compression stockings that you are getting are latex-free.
What are the causes of swelling in leg?
Leg swelling is a common condition. It is referring to excessive buildup of fluid in the leg. Both men and women of all ages are equally affected. It can occur in one or both legs depending on the cause. There are many reasons why legs can be swollen. It is crucial to find out the causes as some of them may be serious and life-threatening.
The common causes of leg swelling include the following:
1. Venous insufficiency
Venous insufficiency is a very common cause of leg swelling. Failure of valves (Varicose veins) or damage of valves (from previous deep vein thrombosis (DVT)) in the leg veins will prevent the blood in the veins from travelling back towards the heart effectively. This results in pooling of blood in the veins of the affected leg and hence fluid buildup in the tissue.
2. Heart failure
Failure of heart to pump blood out effectively to all the organs can lead to backlog of blood pooling in the legs and hence buildup of fluid.
3. Kidney failure
Kidney failure will lead to reduced function in filtering wastes and excreting excess fluids from the body. Swelling or fluid retention tend to affect both lower limbs and it may affect arms in more severe cases.
4. Pregnancy
Leg swelling is a normal part of pregnancy. Third trimester, starting from week 28, is the most common period to experience it. This is because the growing baby in the uterus can cause external compression to the pelvic veins, which are major veins that allow blood to return to the heart. However, leg swelling during pregnancy may be a sign of more sinister problem. For example:
- Preeclampsia especially if it is also associated with severe headaches, vision problems and nausea/vomiting
- DVT especially when it is associated with redness and pain in the calf
5. Medications that cause leg swelling
It is important to check the list of medications that you consume as some of them may be associated with leg swelling. For example:
- NSAIDs (Non-steroidal anti-inflammatory drugs) such as Ibuprofen and Voltaren are commonly used to manage pain and inflammation. They are known to be one of the causes because of their salt retention property.
- Oral steroids such as prednisolone are commonly used for severe asthma, severe allergies and autoimmune diseases like rheumatoid arthritis. Leg swelling can occur because of salt retention too especially in prolonged usage.
- High blood pressure medications – medication like amlodipine is known to cause the leg to swell. Do seek help from your doctor to check through your list of medications and modify them as necessary.
The Growing Diabetes Epidemic in Singapore: The Challenges
Diabetes is a growing epidemic in our nation and globally. The prevalence of diabetes among Singapore residents (Singapore citizens and permanent residents) has increased over the past decade. In Singapore, it is estimated that 1 in 9 adults has diabetes. Today, there are over 450,000 Singaporeans living with diabetes. This number is projected to go up to 1 million by 2050 if nothing is done. The Ministry of Health (MOH) launched the War on Diabetes in 2016 in response to the significant health and societal burden posed by diabetes. The cost burden of diabetes, including loss of productivity, is anticipated to double from S$940 million in 2014 to S$1.8 billion in 2050.
People with diabetes are at high risk of developing a range of serious complications, including heart disease, kidney failure, blindness, and lower-extremity complications. The most disabling of these is the lower limb complications. It is the leading cause of diabetes-related hospitalisations and lower limb amputations. In addition to high healthcare costs, it is also associated with a significant reduction in quality of life.

Diabetes Complications
Diabetic Foot Complications
Approximately 25% of diabetics will develop a foot wound or ulcer in their lifetime. Amputation in people with diabetes is 10 to 20 times more common than in people without diabetes. Every year, more than one million leg amputations are performed globally because of diabetes, which is equivalent to one leg amputation every 30 seconds.
In a person with diabetes, higher than normal sugar levels in the body will, over time, damage nerves (neuropathy) and cause blood vessels of the leg and foot to narrow and harden (atherosclerosis), leading to reduced blood flow down to the feet (Peripheral Arterial Disease (PAD)).
a) Diabetic neuropathy:
Diabetic neuropathy can lead to
i) Poor sensation in the feet: Minor injuries to the foot can be left undetected because of poor sensation and may consequently lead to foot ulceration and infection.
ii) Foot deformities: Structural changes in the foot, such as hammertoes, claw toes, the collapse of the midfoot (Charcot’s foot), and limited joint mobility, can result in focal areas of high pressure on the sole. Skin can break down over pressure points, leading to ulceration.
iii) Decreased sweating: Nerves supplying the sweat glands stop functioning, leading to dry, flaky, and cracked skin. Cracked skin in the foot may allow bacteria to enter and cause infection.
b) Peripheral Arterial Disease (PAD):
People with diabetes are at increased risk of atherosclerosis, which narrows and hardens the blood vessels of the leg and within the foot. Poor blood supply to the foot will lead to poor healing and gangrene, as well as a reduced ability to fight infection.

Atherosclerosis with narrowing of an artery
Here are some statistics on diabetic peripheral arterial disease:
- 70% of diabetic wounds have associated PAD
- An ulceration precedes nearly 85% of diabetes-related amputations. This implies that the majority of the amputations can be prevented.
- Two-thirds of elderly patients undergoing amputation do not return to independent life
- About 70% of amputees will die within 5 years
c) Immunocompromised: A poor immune system reduces the ability to combat infection. Small injuries to the foot, such as cuts, blisters, and ingrown toenails, can become infected easily if left untreated. The combination of neuropathy, PAD and poor immunity is responsible for the increased risk of developing foot complications such as ulcers, gangrene, and infection, which may eventually lead to leg amputation if treatment is not sought early.

Skin cracks

Callus
Diabetic foot deformity Photos


Hammer toes


Claw toes

Flat foot

Amputation

Diabetic Foot Wounds and Ulcers

Gangrene

Infected Wounds

Neuropathic (Pressure) Ulcers
Management of Diabetic Foot Complications
It is important to recognize that most diabetic foot complications are manageable, and amputation can be prevented if treatment is sought early. Delayed treatment of diabetic foot complications is common. The main reasons are an underestimation of the severity of foot problems and a lack of recognition of poor circulation. Management of diabetic foot problems is often complex, and experts from other specialities, including vascular/ endovascular surgery, diabetology, and podiatry, may need to be involved.
Successful management of diabetic foot ulcers/wounds hinges on addressing the following treatment modalities:
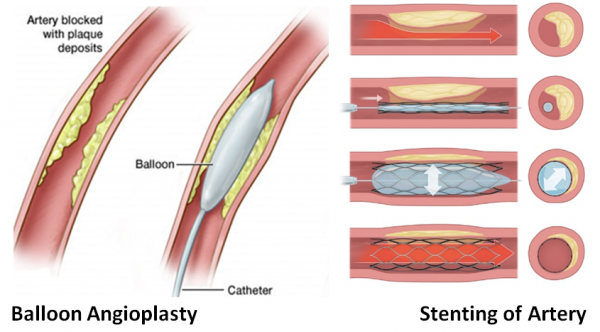
- Ensure adequate blood supply to the foot. Every foot ulcer/wound should be examined for the presence of ischaemia. If poor circulation of the foot is suspected, investigations such as an ultrasound scan or CT angiogram are required to assess the nature of the blockage in the leg arteries. Procedures to improve blood supply to the leg include surgical bypass or endovascular techniques (balloon angioplasty with or without a stent). The treatment of choice depends on the specific type of blockage, which artery is involved, and the general health condition of each patient.
- Control of infection: Signs of wound infection may include:
- Peri-wound redness or swelling
- A foul-smelling wound
- Pus
- Pain
Systemic signs of infection may include fatigue, fever, tachycardia (an increased heart rate), and general malaise. When infection is clinically present, cultures should be obtained. Depending on the infection’s severity, antibiotics shown to be effective against the offending bacteria through sensitivity testing should be given either orally or intravenously.
For a severe wound infection with significant tissue destruction involving muscle, tendon, and bone; urgent surgical intervention will be needed to control the spread of the infection.
- Wound care
- Debride all non-viable tissue (e.g. callus, foreign bodies and necrotic tissue) that may impede wound healing
- Appropriate dressing choice to ensure a moist wound environment for healing.
- Antimicrobial dressings need to be considered to treat and prevent wound infection
- Offloading: redirecting weight (or pressure) off and away from the wound with proper footwear. Some patients may require wheelchairs or crutches to achieve effective offloading.
Prevention
Management of risk factors
- Blood sugar level: High blood sugar, the hallmark of diabetes, injures nerves and blood vessels throughout the body.
- High blood pressure: high blood pressure damages blood vessels, leading to atherosclerosis
- High cholesterol levels and the accumulation of cholesterol-rich fatty deposits in arteries can result in atherosclerosis.
Lifestyle modification
- Smoking cessation: Smoking interferes with blood circulation, and so compounds the effects of nerve and blood vessel damage.
- Exercise naturally improves circulation while working to lower cholesterol and improve heart function.
- Healthy diet: Avoiding excessive salt and saturated fats can help you manage your body weight, blood pressure, and cholesterol.
- Weight loss improves the body’s ability to control blood sugar and takes some pressure off the feet.
Foot Care
- Check your feet and toes every day for cuts, sores, corns or blisters
- Never go barefoot. Choose shoes that are comfortable and fit well. Ill-fitting shoes can cause corns and calluses, ulcers, and nail problems.
- Wash your feet daily. Apply moisturising skin lotion to feet to prevent dryness and cracks.
- Cut or file your toenails regularly.
- Yearly foot screening by a podiatrist, doctor, or trained nurse: Early identification of those at risk of diabetic foot ulcers will prevent the development of foot complications and thus reduce the number of amputations.Education on proper foot care and good glycaemic (blood sugar level) control

Finally, if there are symptoms of unusual pain, redness in the foot, swelling, injury to the foot, infection, or ulcer; make sure this is checked by your doctor or diabetic nurse as soon as possible. There is a clear need to recognise decreased perfusion or vascular impairment as an indicator of the need for revascularization in the diabetic foot in order to achieve and maintain healing and to avoid or delay a future amputation. Early identification of the problem and treatment before it becomes severe is CRITICAL to preventing limb loss.
Why do pregnant women get varicose veins?
Up to 70% of pregnant women suffer from varicose veins in the legs during pregnancy. Varicose veins are enlarged veins that appear to be bulging, tortuous, and bluish in colour, running just underneath the skin. Veins in the legs have one-way valves, which ensure blood flows from the feet towards the heart in one direction. Failure of one-way valves in the leg veins will allow blood to flow backward towards the feet, stretching the walls of the veins. Some pregnant women are especially prone to developing varicose veins when they have a family history of varicose veins, are overweight, or have a job that requires prolonged standing or sitting. Pregnancy can also exacerbate the symptoms of those who already have varicose veins.

Vein with normal working valve

Vein with normal working
There are various reasons that may account for the development of varicose veins during pregnancy:
- An increase in pregnancy hormones (oestrogen and progesterone) will lead to dilatation of veins and failure of one-way valves in the veins to work properly
- The enlarging uterus of a growing baby may result in compression of pelvic veins, which are responsible for returning blood from legs to the heart
- An increase in total blood volume during pregnancy to support a growing baby will lead to stretching of the vein wall. An increase in the diameter of veins will prevent one-way valves from closing properly, leading to the pooling of blood in the legs.
What are the symptoms?
Symptoms of varicose vein in the leg may include:
- Swelling feet and ankles: Swelling tends to be more significant during the late stage of pregnancy and especially worse towards the end of the day. This is due to the pooling of blood in the leg because of gravity and vein valve failure.
- Heaviness
- Tiredness
- Aches
- Pain- may be burning, crampy, throbbing or shooting in nature
- Muscle cramps at night
- Itching
In addition, pregnant women are up to five times more likely to develop deep vein thrombosis (DVT) than when not pregnant. This is because:
- Blood clots more easily during pregnancy
- Blood flow in the leg veins is also slowed down by the compression of the pelvic veins from the increasing size of the uterus. This encourages the blood to clot.
What is the management of varicose veins during pregnancy?
Surgery or minimally invasive procedures to treat varicose veins should be avoided during pregnancy. Regression of varicose veins is often observed within the first three months after delivery. There are, however, many conservative approaches that can manage varicose vein symptoms effectively during pregnancy:
- Avoid prolonged standing and sitting
- Engage in exercise regularly, such as walking and swimming
- Wear graduated compression stockings. The pressure exerted by the stockings on the leg veins will help the vein valves work properly by promoting blood flow from the leg towards the heart
- Elevate legs regularly to improve venous circulation of the legs
- Try to keep body weight within recommended limits
What is the management of varicose veins during pregnancy?
Surgery or minimally invasive procedures to treat varicose veins should be avoided during pregnancy. Regression of varicose veins is often observed within the first three months after delivery. There are, however, many conservative approaches that can manage varicose vein symptoms effectively during pregnancy:
- Avoid prolonged standing and sitting
- Engage in exercise regularly, such as walking and swimming
- Wear graduated compression stockings. The pressure exerted by the stockings on the leg veins will help the vein valves work properly by promoting blood flow from the leg towards the heart
- Elevate legs regularly to improve venous circulation of the legs
- Try to keep body weight within recommended limits
Conclusions
Do not hesitate to consult a vascular surgeon about your varicose veins, especially when they become symptomatic as pregnancy progresses. It is important to exclude serious conditions, such as DVT. Not uncommonly, varicose veins stay after pregnancy as the valves in the veins are irreversibly damaged. Medical intervention may be required to normalise the vein circulation.
Dr Tan Yih Kai, a Senior Consultant Vascular and Endovascular Surgeon at The Vascular Vascular Vein and Wound Centre is a leading specialist in the care of varicose veins. He has many years of experience treating patients with varicose veins and the associated complications, such as DVT.
Welcome to our comprehensive guide on venous leg ulcers. In this article, we will delve into the causes, symptoms, treatment options, and prevention strategies for venous leg ulcers. Venous leg ulcers are a common condition that affects a significant number of individuals worldwide. Understanding this condition is crucial for effective management and prevention. So, let’s dive in and explore the world of venous leg ulcers.
Venous Leg Ulcers
Venous leg ulcers refer to open sores that develop on the legs due to impaired blood flow. They typically occur because of chronic venous insufficiency, a condition where the veins in the legs fail to adequately return blood back to the heart. This can lead to a buildup of pressure in the veins, causing fluid leakage and the formation of ulcers.
Causes of Venous Leg Ulcers
Several factors contribute to the development of venous leg ulcers. The primary cause is chronic venous insufficiency, which is often a result of damaged or weakened valves in the leg veins. Other common causes include:
- Deep vein thrombosis (DVT): Blood clots that form in the deep veins of the legs can obstruct blood flow and lead to ulcers.
- Varicose veins: Swollen and twisted veins can hinder blood circulation, increasing the risk of ulcers.
- Obesity: Excess weight puts additional pressure on the veins, impairing their function.
- Inactivity: Sitting or standing for long periods can hamper blood flow, contributing to ulcers.
- Previous leg injuries: Trauma or surgery to the leg can damage the veins, leading to ulcers.
- Age: The risk of venous leg ulcers increases with age.
Symptoms of Venous Leg Ulcers
Venous leg ulcers present with specific symptoms that help distinguish them from other types of leg sores. If you notice any of the following signs, it is essential to seek medical attention:
- Open sores or wounds on the legs that are slow to heal.
- Irregularly shaped ulcers with a shallow depth.
- Surrounding skin discoloration, often with a reddish-brown hue.
- Swelling in the affected leg.
- Pain or discomfort, especially when standing or walking.
- Itching or a feeling of heaviness in the leg.
It is important to note that venous leg ulcers can cause significant distress and impact an individual’s quality of life. Seeking early diagnosis and appropriate treatment is crucial for effective management.
Diagnosing Venous Leg Ulcers
When you consult a healthcare professional for suspected venous leg ulcers, they will conduct a thorough examination and evaluate your medical history. Diagnostic tests and procedures may include:
- Doppler ultrasound: This non-invasive test helps assess blood flow in the leg veins and identifies any obstructions or abnormalities.
- Blood tests: These tests can help rule out other underlying conditions that may contribute to ulcer formation.
- Wound culture: A sample of the wound may be collected and tested to identify any infection.
Once a diagnosis of venous leg ulcers is confirmed, your healthcare provider will recommend a suitable treatment plan based on the severity of the ulcers and your overall health.
Treatment Options for Venous Leg Ulcers
Treating venous leg ulcers typically involves a combination of strategies aimed at promoting wound healing, managing symptoms, and addressing the underlying cause. The following treatment options are commonly employed:
- Compression Therapy
Compression therapy is a cornerstone in the treatment of venous leg ulcers. It involves applying pressure to the affected leg using compression bandages or stockings. This helps improve blood circulation, reduce swelling, and promote healing. Compression therapy should be tailored to each individual’s needs and may require regular adjustments by a healthcare professional.
- Wound Dressings
Proper wound care is essential for venous leg ulcer healing. Various types of dressings are available, including hydrocolloids, foams, and alginate dressings. These dressings create a moist environment that promotes granulation and reduces the risk of infection. It is important to change dressings regularly and follow healthcare provider instructions for optimal wound care.
- Medications
In some cases, medications may be prescribed to manage symptoms and support healing. These may include:
- Topical ointments or creams: Antiseptic or antimicrobial agents can help prevent infection and promote healing.
- Pain medications: Over-the-counter or prescription pain relievers may be recommended to alleviate discomfort associated with venous leg ulcers.
- Antibiotics: If an infection is present, antibiotics may be prescribed to treat the underlying bacterial growth.
It is crucial to follow the prescribed medication regimen and inform your healthcare provider of any adverse effects or concerns.
- Debridement
Debridement involves the removal of dead or unhealthy tissue from the wound bed. This can be done through various methods, such as surgical debridement, enzymatic debridement, or autolytic debridement. Debridement helps facilitate healing by promoting the growth of healthy tissue.
- Surgical Intervention
In some cases, surgical intervention may be necessary, particularly if the venous leg ulcers are large, chronic, or unresponsive to other treatments. Surgical options may include skin grafting, where healthy skin is transplanted to the ulcer site, or venous bypass surgery, which redirects blood flow to bypass damaged veins.
- Lifestyle Modifications
Making certain lifestyle changes can complement medical treatments and prevent the recurrence of venous leg ulcers. These modifications may include:
- Regular exercise: Engaging in activities that promote leg muscle movement can enhance blood circulation.
- Weight management: Maintaining a healthy weight reduces the strain on the veins.
- Leg elevation: Elevating the legs above heart level whenever possible helps alleviate swelling and promote blood flow.
- Avoiding prolonged sitting or standing: Taking breaks and avoiding prolonged periods of inactivity can reduce the risk of venous insufficiency.
Conclusion
Venous leg ulcers are a common condition that can significantly impact an individual’s quality of life. Understanding the causes, symptoms, treatment options, and prevention strategies is crucial for effective management. If you suspect you have venous leg ulcers, it is important to seek medical attention for a proper diagnosis and personalized treatment plan. By following the recommended treatments, making lifestyle modifications, and maintaining regular follow-ups with your healthcare provider, you can improve healing outcomes and reduce the risk of recurrence.
Remember, each case of venous leg ulcers is unique, and the information provided in this article is for educational purposes only. Consult with a qualified healthcare professional for personalized advice and guidance.
Frequently Asked Questions (FAQs)
Q1: Can venous leg ulcers be prevented? A1: While not all cases of venous leg ulcers can be prevented, certain measures can reduce the risk. These include maintaining a healthy lifestyle, managing underlying conditions such as diabetes or obesity, and wearing compression stockings if recommended by a healthcare professional.
Q2: How long does it take for venous leg ulcers to heal? A2: The healing time for venous leg ulcers varies depending on factors such as the size and severity of the ulcer, adherence to treatment, and individual healing capacity. In general, venous leg ulcers may take several weeks to several months to heal completely.
Q3: Are venous leg ulcers contagious? A3: No, venous leg ulcers are not contagious. They are caused by impaired blood flow and underlying venous insufficiency, not by any infectious agent.
Q4: Can I shower or bathe if I have venous leg ulcers? A4: It is generally safe to shower or bathe if you have venous leg ulcers. However, it is important to protect the wound from excessive moisture and follow the guidance.
provided by your healthcare professional. They may recommend using a waterproof dressing or taking precautions to keep the wound dry during bathing.
Q5: Are there any alternative therapies or home remedies for venous leg ulcers? A5: While it is important to consult with a healthcare professional for appropriate treatment, there are certain measures you can take at home to support the healing process. These include maintaining good hygiene, keeping the legs elevated, avoiding excessive heat or cold on the affected area, and following a nutritious diet to promote overall health.
Q6: Can I continue my daily activities with venous leg ulcers? A6: It depends on the severity of your condition and the recommendations of your healthcare provider. In many cases, individuals with venous leg ulcers can continue their daily activities while following certain precautions. It is important to avoid activities that put excessive pressure or strain on the legs and to take breaks to elevate the legs when needed.